Guide to Testosterone Replacement Therapy

Testosterone replacement therapy may be prescribed for those with low testosterone levels. However, this treatment has known detrimental impacts on sperm production. Read on to learn more about what TRT is, how it affects your body, and what you can do to protect your fertility.
What is testosterone replacement therapy (TRT)?
Testosterone replacement therapy (TRT) is a treatment for low testosterone, also known as male hypogonadism. Testosterone is a sex hormone that’s essential for the body; it’s produced in the testicles. In men, it’s necessary for:
- sperm production
- fertility
- sex drive
- sexual development, such as testicular development and descent
- defining male secondary sexual characteristics, such as voice deepening and muscle growth
- healthy bone mass and fat distribution
TRT increases the levels of testosterone in your blood using testosterone that was manufactured in a lab. The goal is to reach and maintain normal testosterone levels while relieving symptoms of low-T and improving your quality of life.
TRT is used by around 0.9-2.9% of cis men in the US, and its usage continues to grow. There are both potential benefits and risks to TRT. Current research supports treating younger individuals who have low testosterone. However, using it for older adults, where low testosterone is a common condition, is still under debate.
A form of testosterone therapy can also be used by trans men to develop and maintain typically masculine features. In this article, we’ll be primarily discussing people who produce sperm.
Methods of administering testosterone therapy
- Testosterone injection: An injection of testosterone into the muscle may be needed every 2–3 weeks or up to every 3 months, depending on the type used. Injections are usually cheaper than other forms of TRT but also have a higher chance of side effects. They may be self-administered.
- Testosterone patch. This delivers testosterone continuously for 24 hours, but you’ll usually need to apply it every day. While the scrotum has a higher absorption rate, it tends to be easiest to place the patch on your back, thigh, stomach, or upper arm. Skin irritation is more common with a patch.
- Implant. Testosterone pellets may be implanted under the skin of your stomach or in the buttock muscle. The pellets last for about 4-7 months, but a new procedure is needed each time to replace them, and there’s a chance of infection.
- Testosterone gel. Usually contains 1% testosterone, applied daily to your shoulders, stomach, or upper arm. You’re less likely to experience skin irritation than when using a patch, but should be careful that the gel doesn’t come in contact with other people, such as your partner or children. An advantage of gels is that the dose can easily be changed if necessary.
- Nasal gel. This newer form of TRT comes as a gel that you squirt into your nostrils. You’ll typically use it three times per day.
- Buccal tablet. You place a tablet between your gums and cheek, which will slowly absorb the testosterone. You’ll need to keep a tablet in your mouth for a full day, which can be difficult for many people.
- Oral tablet or capsule. In 2019, the FDA approved an oral testosterone capsule containing testosterone undecanoate to treat hypogonadism related to certain medical conditions. However, other types of oral testosterone can cause liver damage, and aren’t recommended for TRT.
What is low testosterone/male hypogonadism?
A healthy testosterone level for most men is between 300 ng/dL and 1,000 ng/dL, when measured via a blood test in the morning. (Testosterone should always be measured between 7 and 11 am, since this is when it’s at its highest level.) Younger men typically have a testosterone level of 600–900 ng/dL while older men are around 500–800 ng/dL.
Low testosterone, also called low-T or male hypogonadism, occurs when your body produces an insufficient amount of the testosterone hormone. In middle-aged and older men, it’s referred to as late-onset hypogonadism.
Research indicates that around 39% of men aged 45 or above experience hypogonadism, but only between 5 and 35% of them are treated.
There are two types of hypogonadism, which can be categorized depending on their cause. If you have low testosterone, you may have either one or both types.
- Primary hypogonadism is low testosterone caused by a problem with the testicles. This may result in low testosterone levels with high concentrations of luteinizing hormone (LH) and follicle stimulating hormone (FSH).
- Secondary hypogonadism is low testosterone caused by an issue in the hypothalamus or pituitary gland, the areas in your brain that produce hormones to tell your testicles to make testosterone. This causes low testosterone levels along with low or normal levels of LH and FSH.
After a blood test has confirmed low testosterone levels, measuring your LH and FSH levels can help identify whether you have primary or secondary hypogonadism.
Causes of low testosterone
- Klinefelter’s syndrome, a genetic disorder which leads the testicles to develop abnormally and produce less testosterone
- Kallmann syndrome, a genetic disorder which causes issues with hypothalamus development, resulting in low testosterone levels
- mumps infection that affects the testicles
- undescended testicle, which may affect testosterone and sperm production if it isn’t fixed at a young age
- chemotherapy or other cancer treatments
- taking certain medications
- injuring the testicles
- tuberculosis
- liver failure
- HIV/AIDS
- obesity
- aging, with a decline in testosterone levels of around 1% per year after age 30
- stress
- over-exercising
Symptoms of low testosterone
If you have low-T, you may have no symptoms, or they may include:
- low sex drive
- erectile dysfunction
- low sperm count — Check your sperm count with an at-home semen analysis
- depression
- difficulty sleeping
- having trouble concentrating
- hot flashes
- breast discomfort
- decreased testicle size
- reduced muscle mass and strength
- lower bone mass (osteoporosis occurs twice as much in men with low-T compared to those with a normal level of testosterone)
- increased body fat
Many of these symptoms may be similar to those caused by other conditions (like high blood pressure) or by older age. This can make them difficult to notice and treat.
Diagnosing low testosterone
Low testosterone may be suspected due to symptoms, and confirmed with blood testing. A blood test will measure the main types of testosterone:
- free testosterone, which isn’t attached to proteins and can be used by the body
- albumin-bound testosterone, which is weakly attached to the protein albumin and can likely also be easily accessed by your body
- sex hormone binding globulin (SHBG)-bound testosterone, which makes up about 44% of testosterone and can’t be easily used by the body
“Total testosterone” is, as it sounds, the total of all three types of testosterone.
You may be diagnosed with hypogonadism if you have less than 300 ng/dL of total testosterone in your blood after repeated testing, and show at least one other symptom.
You may also receive a diagnosis of hypogonadism if your total testosterone levels are normal, but you still have symptoms. In fact, research suggests that low levels of free testosterone may be linked to erectile dysfunction, even if total testosterone levels are within the standard range.
How testosterone replacement therapy can help
If you have low testosterone, increasing your testosterone levels to the normal range can improve low-T symptoms, resulting in:
- improved sex drive
- enhanced mood and energy levels
- improved sexual function
- increased red blood cell production
- decreased body fat
- higher bone mineral density
- improved cognition
Improvements in sex drive and mood typically occur soon after beginning TRT. You’ll likely experience a decrease in body fat and increased bone mineral density within 6 months of starting treatment. You may continue to see benefits after a longer period of TRT.
If your symptoms don’t show improvement after 3 months of TRT, your doctor will likely reevaluate the potential causes behind your condition.
Side effects of testosterone replacement therapy
There’s limited evidence about the potential side effects of testosterone replacement therapy, especially when used long-term. The following are possible issues:
- liver damage
- erythrocytosis (excessively high production of red blood cells)
- infertility (for this reason, you may consider sperm freezing before TRT)
- enlarged prostate
- trouble sleeping
- blood clots
Testosterone replacement therapy may have additional side effects, but more research is needed to confirm them. These include possible increased risks of heart attack and cancer.
TRT and heart attack risk
Using TRT comes with a potential increased risk of heart attack, stroke, and myocarditis (inflammation of the heart). As research has particularly linked this issue to older men, it’s an important factor to take into account for TRT patients over the age of 55, who are already at increased risk.
A large 2014 study found an increased risk of heart attack in men aged 65 and above as well as in younger men with heart disease after taking TRT. The study noted that taking testosterone may increase blood clotting and blood pressure, which may contribute to heart attacks.
Another study also showed a higher chance of negative cardiovascular events among older men who were using testosterone gel. Many of these men also had other chronic diseases.
On the other hand, some recent research has suggested that TRT may reduce cardiovascular risks in men with very low testosterone levels. Compared to participants who did not receive treatment, men younger than 55 who used TRT had a 25% lower chance of heart attack and stroke, while men over 60 on TRT had a 15% lower risk. The men using TRT also had health improvements in other areas.
In another study, testosterone was even used as a treatment for cardiovascular issues, improving exercise capacity in men with heart failure. Only 24% of participants had low testosterone levels when they began the study.
More research is needed to evaluate the risk of TRT on heart conditions. For the moment, the FDA requires that prescription testosterone product labels include warnings of the potential higher chance of strokes and heart attacks. It’s important to seek immediate medical care if you experience any of the following, particularly while taking testosterone:
- difficulty breathing
- pain in your chest
- slurring while speaking
- weakness in one area of your body
TRT and cancer risk
There’s some concern that TRT may heighten the risk of prostate cancer because testosterone promotes the growth of prostate cancer cells. However, little, if any, research supports this. While more research should be done in this area, multiple studies and analyses indicate that TRT does not impact prostate cancer risk.
A recent study of over 12,000 men with late-onset hypogonadism found that using TRT was not linked to a higher chance of prostate cancer. All of the men were at least 45 years old with no history of prostate cancer, and many had a follow-up period of multiple years.
Research from 2017 also found no elevated risk of prostate cancer, even after participants received TRT for a longer period. In fact, those who took TRT had a lower chance of aggressive prostate cancer.
Similarly, a meta-analysis indicated that using TRT did not cause an increase in prostate cancer compared to controls. It also found no increase in prostate-specific antigen (a marker that tends to be elevated when prostate cancer is present) related to TRT, except for a slight increase with testosterone injections.
More research is needed to confirm the link, or lack thereof, between TRT and cancer. It’s currently recommended that individuals receiving TRT undergo regular checks for prostate cancer. Additionally, you shouldn’t use TRT if you already have prostate cancer.
Can I use TRT if I have normal testosterone levels?
Studies show that prescriptions of TRT for off-label use have expanded, leading to patients receiving prescriptions for testosterone even if they don’t have hypogonadism or if blood testosterone levels have not been assessed. In up to around 25% of cases, men receiving testosterone may not have had their testosterone levels checked before starting therapy. As of 2017, 3 out of 1,000 male military service members were being inappropriately treated with TRT.
People may also take testosterone without receiving a prescription. Anabolic-androgenic steroids contain synthetic versions of testosterone that can be injected into muscles, taken orally, or used as a gel or cream. Some athletes — primarily men — use these steroids to enhance their physical performance or build muscle mass.
Testosterone is an important treatment for some medical conditions, but it shouldn’t be taken recreationally. Non-medical doses can be 10 to 100 times higher and may lead to a range of health problems, including:
- liver damage
- kidney problems
- higher risk of blood clots
- reduced sperm count
- baldness
- high risk of prostate cancer
Using anabolic-androgenic steroids may also reduce natural testosterone production. According to research, previous use of steroids is the most common cause of profound hypogonadism — nearly non-existent testosterone levels — in men under 50.
Testosterone replacement therapy and fertility
Testosterone plays an essential role in spermatogenesis (sperm production), primarily through helping control processes including meiosis (cell division) and the release of mature sperm. However, testosterone levels are between 25 and 125 times higher in the testes than in the blood, so even if you have low blood testosterone levels, you still likely have enough for sperm production.
Testosterone is an important hormone for male fertility, but boosting your testosterone levels doesn’t translate to increased fertility. In fact, the opposite is true. Injecting exogenous (external) testosterone will disrupt the hormone balance and actually halt sperm production — something that’s important to consider if you’re interested in trying TRT.
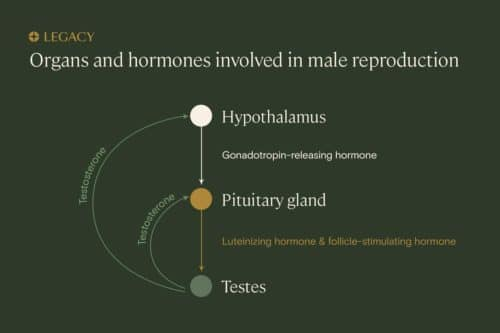
Testosterone and the hypothalamic-pituitary-gonadal axis
Several parts of your body work together to keep your reproductive system functioning normally. This system is called the hypothalamic-pituitary-gonadal axis.
An area of your brain called the hypothalamus releases gonadotropin-releasing hormone (GnRH), which stimulates the pituitary gland to release follicle-stimulating hormone (FSH) and luteinizing hormone (lH). In turn, FSH and LH impact the functions of the testicles. FSH controls the maturation and function of Sertoli cells, which play a critical role in sperm production. Meanwhile, LH is needed for the testes to make testosterone.
Finally, the testosterone created by the testicles does a “feedback loop” back to the brain to turn on — or off — GnRH, FSH, and LH production. This is one of many hormone “cascades” in the human body.
Changes within the system affect other parts of it. When you increase your blood testosterone levels by taking testosterone, your hypothalamus and pituitary glands respond by shutting down production of the hormones that are vital for sperm production. Research shows that TRT causes suppression of FSH and LH to abnormally low levels — less than one-half of their original levels in the men studied.
TRT and sperm production
Because taking exogenous testosterone reduces FSH and LH, it also impairs sperm production and fertility. Testosterone has actually been studied for use as a male contraceptive, resulting in azoospermia (lack of sperm in semen) within 4 months in 65% of men with previously normal sperm counts.
While TRT can improve sexual function, it also reduces fertility, presenting a difficult choice for individuals with symptoms of hypogonadism who want to have children. If you’re currently trying to conceive, you should not use TRT or should stop using it immediately. You can also consider sperm freezing before TRT.
Is the effect of TRT on male fertility reversible?
Because the dose of testosterone in anabolic steroids is so high, it’s been shown to permanently halt sperm and testosterone production in the testes.
However, TRT is typically a much lower dose, and is therefore not likely to permanently affect your fertility. Research shows that sperm production typically recovers within 1 year after men stop taking testosterone; in some men, it may take as long as 2 years. However, restored sperm counts aren’t a guarantee, and are less understood for older individuals and those using TRT long term. One to two years may also be longer than some people wish to wait to conceive.
Can hCG prevent TRT from affecting fertility?
It may be possible to reduce the impact of TRT on fertility. Human chorionic gonadotropin (hCG), also known as the “pregnancy hormone” because it’s produced during pregnancy, mimics the effect of LH in the body, prompting the testes to continue to produce their own testosterone.
Taking hCG alongside TRT may help offset the effect of exogenous testosterone on sperm production. Research has indicated that taking hCG alongside TRT maintained intratesticular testosterone at normal levels, though it noted that more studies need to be done on sperm production under these conditions. A subsequent study examined this issue, finding that hCG seemed to preserve semen parameters, and potentially fertility, during TRT.
Taking hCG may also allow for a quicker restoration of sperm counts following TRT. According to one study of men who had very low sperm counts while using testosterone, taking 3,000 units of hCG every other day after stopping TRT improved sperm counts in 95.9% of participants over an average of 4.6 months — a shorter period than typically achieved without hCG.
Your doctor may prescribe hCG along with TRT. However, it’s once again not guaranteed to preserve or recover sperm production.
Sperm freezing is the best way to protect your fertility before TRT
If you’ve been diagnosed with low-T and you want biological children in the future, the best thing you can do to protect your fertility options is to freeze some sperm. Sperm freezing is the process of using liquid nitrogen to preserve one or more sperm samples for possible use later on.
It’s a fairly simple process. First, you produce a semen sample via masturbation. This sample is then assessed under a microscope in a semen analysis, to determine if your sperm are healthy and viable for freezing. Finally, sperm are plunged into liquid nitrogen to freeze them at a temperature of -196ºC — the temperature at which biological activity pauses — and transferred to liquid nitrogen storage tanks to maintain their low temperature.
Once frozen, your sperm can be stored indefinitely without a decrease in quality or likelihood that it will create a pregnancy. Frozen sperm can be used in intrauterine insemination (IUI), the “turkey baster” method, as well as IVF, a process in which eggs and sperm are combined outside the body in a lab. Learn more about sperm freezing.

Legacy makes the sperm freezing process even easier with at-home semen analysis and sperm freezing kits.
Should I try TRT?
According to the FDA, TRT should only be used by men whose low testosterone levels are a result of medical conditions. Doctors sometimes prescribe testosterone therapy for individuals who have lower testosterone due to their age, and some research as well as the 2018 Endocrine Society Clinical Practice Guidelines support this for men over 65 who have both low testosterone levels and related symptoms. However, you should be aware that this is currently not an approved use by the FDA.
TRT may be a good option for you if:
- you have a diagnosis of low testosterone (below 300 ng/dL after at least two separate tests)
- you have multiple symptoms of low testosterone
- you've already had children or don’t want children (or you freeze your sperm)
You should not start TRT if you have:
- polycythemia (blood cancer)
- prostate cancer
- 50% or higher volume of red blood cells in your blood
- untreated obstructive sleep apnea
- experienced a heart attack or stroke in the previous 6 months
- plans to have children soon or in the future
References
- Nazem Bassil et al. "The benefits and risks of testosterone replacement therapy: a review." Therapeutics and Clinical Risk Management, 2009.
- “FDA approves new oral testosterone capsule for treatment of men with certain forms of hypogonadism.” FDA, 2019.
- Eric Larsen, MD et al. "Testosterone Replacement Therapy Use Among Active Component Service Men, 2017." Military Health System, 2019.
- Christos P Tsametis et al. "Testosterone replacement therapy: For whom, when and how?" Metabolism, 2018.
- Jacob Rajfer, MD. "Decreased testosterone in the aging male." Reviews in Urology, 2003.
- Jathin Bandari et al. "Marketing and Testosterone Treatment in the USA: A Systematic Review." European Urology Focus, 2017.
- "Anabolic Steroids DrugFacts." National Institute on Drug Abuse, 2018.
- Ylenia Duca et al.”Substance abuse and male hypogonadism.” Journal of Clinical Medicine, 2019.
- Omeed Sizar et al. "Hypogonadism." StatPearls, 2021.
- P Dandona et al. “A practical guide to male hypogonadism in the primary care setting.” International Journal of Clinical Practice, 2010.
- Peeyush Kumar et al. "Male hypogonadism: Symptoms and treatment." Journal of Advanced Pharmaceutical Technology & Research, 2010.
- Chaoyang Li, MD, PhD et al. "Association of Testosterone and Sex Hormone–Binding Globulin With Metabolic Syndrome and Insulin Resistance in Men." Diabetes Care, 2010.
- Yan-Ping Huang et al. "Free testosterone correlated with erectile dysfunction severity among young men with normal total testosterone." International Journal of Impotence Research, 2019.
- "Could you have low testosterone?" MedlinePlus, 2021.
- William D. Finkle et al. "Increased Risk of Non-Fatal Myocardial Infarction Following Testosterone Therapy Prescription in Men." PLOS One, 2014.
- Shehzad Basaria et al. "Adverse events associated with testosterone administration." The New England Journal of Medicine, 2010.
- "Testosterone therapy reduces heart attack and stroke." EurekAlert!, 2021.
- Chris J. Malkin et al. "Testosterone therapy in men with moderate severity heart failure: a double-blind randomized placebo controlled trial." European Heart Journal, 2006.
- "FDA Drug Safety Communication: FDA cautions about using testosterone products for low testosterone due to aging; requires labeling change to inform of possible increased risk of heart attack and stroke with use." FDA, 2015.
- Abraham Morgentaler, MD. "Testosterone Replacement Therapy and Prostate Cancer." Urologic Clinics of North America, 2007.
- Christina Santella et al. "Testosterone Replacement Therapy and the Risk of Prostate Cancer in Men With Late-Onset Hypogonadism." American Journal of Epidemiology, 2019.
- Stacy Loeb et al. "Testosterone Replacement Therapy and Risk of Favorable and Aggressive Prostate Cancer." Journal of Clinical Oncology, 2017.
- De-Ying Kang et al. "The effect of testosterone replacement therapy on prostate-specific antigen (PSA) levels in men being treated for hypogonadism: a systematic review and meta-analysis." Medicine (Baltimore), 2015.
- Ryan C. Petering, MD et al. "Testosterone therapy: review of clinical applications." American Family Physician, 2017.
- Lee B. Smith et al. "The Regulation of Spermatogenesis by Androgens." Seminars in Cell & Developmental Biology, 2014.
- Catherine E. Klein, MD. "The Hypothalamic-Pituitary-Gonadal Axis." Holland-Frei Cancer Medicine, 2003.
- Amir Shahreza Patel et al. "Testosterone Is a Contraceptive and Should Not Be Used in Men Who Desire Fertility." World Journal of Men's Health, 2019.
- Lindsey E Crosnoe et al. "Exogenous testosterone: a preventable cause of male infertility." Translational Andrology and Urology, 2013.
- John Alden Lee et al. "Indications for the use of human chorionic gonadotropic hormone for the management of infertility in hypogonadal men." Translational Andrology and Urology, 2018.
- Evan P. Wenker et al. "The Use of HCG-Based Combination Therapy for Recovery of Spermatogenesis after Testosterone Use." The Journal of Sexual Medicine, 2015.
- Andrea D Coviello et al. "Low-dose human chorionic gonadotropin maintains intratesticular testosterone in normal men with testosterone-induced gonadotropin suppression." The Journal of Clinical Endocrinology & Metabolism, 2005.
- Tung-Chin Hsieh et al. "Concomitant intramuscular human chorionic gonadotropin preserves spermatogenesis in men undergoing testosterone replacement therapy." The Journal of Urology, 2013.
- Christina Dimopoulou et al. "EMAS position statement: Testosterone replacement therapy in the aging male." Maturitas, 2016.
- Shalender Bhasin et al. "Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline." The Journal of Clinical Endocrinology & Metabolism, 2018.
Find what's right for you
